

Good Intentions, and Bad Arguments for Child Transitioning
Good Intentions, and Bad Arguments for Child Transitioning
On medically transitioning transgender children

The issue of permitting minors to transition toward their preferred identity is a very difficult one, and the difficulties are not unique to transgenderism. You may be in favor of legalizing drugs, but does that mean a 10 year old should be able to buy heroin? You may also be in favor of legalized prostitution, but would you allow a 15 year old to buy a prostitute’s services?
Whatever we may say about adults, issues get more complicated (and emotional!) when we discuss children. Whether to allow children to transition or not is a most difficult topic.
Today, I’d like to take on 2 different (bad) arguments in favor of allowing children to transition. Note that just because bad arguments are made in favor of a conclusion, it does not necessarily mean that the conclusion is wrong, but it means we will need better arguments. It might also make us a bit suspicious, as we can’t help but wonder if this is the best transgender advocates can do.
Deferral to the Experts
Honest liberals understand the difficulties with transgender health services for children. To what extent can a child understand his or her own motivations? How certain is a child of his or her own identity? To what extent can a child meaningfully plan for all the consequences of choosing to transition? How likely is the child to detransition?
We are told however not to worry - we can leave these questions to the experts! Here is an example of what I mean:
https://twitter.com/JillFilipovic/status/1652308296185815042

On the face of it, this seems reasonable, and I applaud the author’s acknowledgement of the uncertain answers to important questions. The author asks, seemingly reasonably, “wouldn’t we prefer to have doctors (read: experts) working on these sorts of questions, rather than politicians?”
Maybe surprisingly, the answer is, “No, we should not prefer doctors to answer these questions.” These are precisely the sorts of questions best suited for politicians and an electorate, not for doctors. 1
Doctors are not experts on transgenderism2. They may be experts on things like the side effects of surgery, or the effects of hormones on the body, but these effects on the body are largely a distraction from the core questions we need to ask.
The results of research into areas such as the effects of female hormones on male bodies will certainly inform the debate, but they cannot resolve the debate. The core questions are questions of morality, of certainty and stability of our identities, and about the degree of autonomy we should afford to young people.
It is important to remember that doctors have no real insights about transgenderism. There is no meaningful test for transgenderism. Medical professionals may ask a patient, “Are you transgender?” If the patient answers in the affirmative, the so-called principle of ‘gender affirming care’ dictates that medical professionals treat the patient as though he or she is transgender. There is no diagnosis, nor even an attempt at one. A doctor may write, “transgender” on your chart, but that is based solely on the patient’s self-report.
We cannot blame doctors too much for this state of affairs - after all, how are they to know whether the patient is in fact transgender? How can they understand the child’s motivation?
I also do not wish to minimize the importance of doctors. Of course, doctors play a crucial role for anyone who wishes to transition, and will continue to play an important role in generating research and data that will help inform this debate. I maintain however that they are not experts in who should be able to transition, or at what age. These are questions for the child, for parents, and for voters.
Unfortunately letting doctors make these decisions reeks of scientism - deference to science when science isn’t the source of truth.
You Have To Pick
An argument I’ve begun to read more frequently goes something like this. Here we might imagine a transgender advocate advising uncertain parents regarding the transition of their son (soon to be daughter):
”Sure, you may not be certain whether allowing Steve to transition to Sue is a good idea. It may turn out to have been a bad idea. However, preventing Steve from transitioning is itself a choice, and one that might also have bad consequences. Since you have to pick one, why not pick the one the child prefers?”
This argument has some superficial appeal, for a few different reasons:
It (correctly) emphasizes that doing nothing is itself a choice.
It (somewhat correctly) attacks the precautionary principle. Of course, I hope advocates here are consistent in their contempt for the precautionary principle…
However, this argument is a bad one. It suggests that choosing to transition is no worse than choosing not to transition. It argues for a certain indifference to the choices a child may make.
Costs and Benefits are Not Symmetric
To see why this argument is so bad, consider two facts in the context of a child determining whether or not to transition:
A child may choose to transition, or not.
A child may have been better off transitioning, or not.
In other words, there is a choice, followed by an outcome. 2 choices, followed by 2 potential outcomes means there are 4 cases to be considered:
The child transitions, and later realizes he made the correct choice.
The child transitions, but later regrets the decision.
The child does not transition, and later realizes he made the correct choice.
The child does not transition, but later regrets the decision.
Let’s look at these in a matrix. We’ll assume we’re dealing with a 16 year-old who is considering medically transitioning, beginning with hormone therapy (our conclusions are likely to be even stronger if we include surgical interventions).
We’re going to assign a score to each outcome, depending on the outcome, and the child’s assessment of that outcome, 2 years later, at the age of 18:
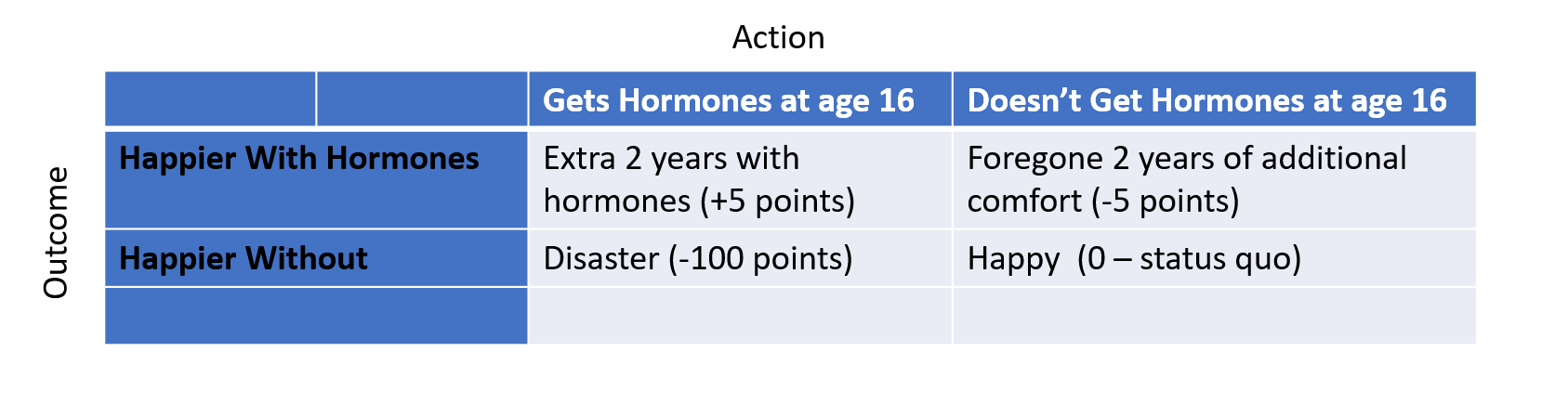
Each column governs a single choice. Let’s start by assuming (probably unrealistically) that the outcomes are 50/50 - our hypothetical patient is approximately as likely to wish he hadn’t transitioned as to wish he had.
Let’s start by looking at the average score of column 1:

Assuming each outcome is equally likely, we see this decision has an average score of -47.5, which is a form of expected value.
Next, let’s look at the average score of column 2:
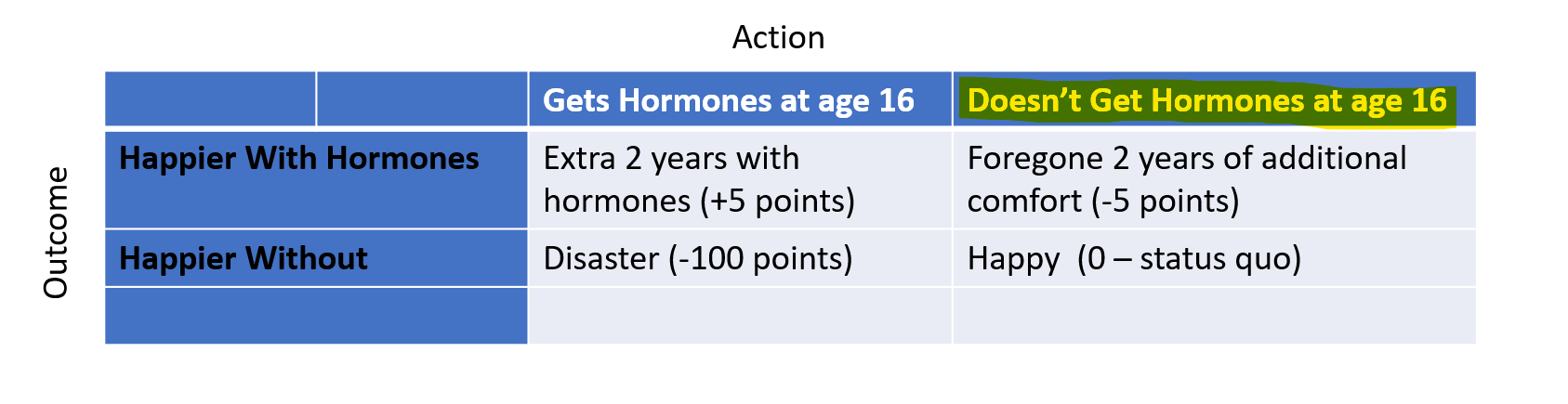
Again, assuming each outcome is equally likely, we get an average score of -2.5 - WAY better than our first score. Sure, he’s marginally worse off if he would have preferred transitioning, but we avoid a potential disaster (transitioning, then later regretting it).
So - how unlikely must regret be in this model before you’d be indifferent to Steve’s transition? If you were concerned only with expected value, you would have to be over 95% certain that Steve would NOT regret transitioning before granting your approval!
Think about your own childhood - how often were you sure you would continue to feel a particular way, only later to decide you didn’t? It’s difficult for teens to be 95% certain about much of anything concerning how they’ll feel in the future.
Model Adjustments
Note that we might be even more heavily weighted toward the choice to wait, simply by changing some assumptions regarding the way we score these outcomes.
The bottom line here is that while it is true that deciding not to transition is itself a choice, it is probably the choice that makes the most sense for the overwhelming percentage of teens and their parents.
If a teen decides not to transition, they can always change their minds down the road, as they gain age and wisdom. However, they cannot go back3, so there is always an option value in waiting.
If you’d prefer, you can evaluate this graph with numbers that are different than mine - I took a rough stab at estimating the relative values of the relevant choices.
Needless to say, a decision to transition that is later regretted is an unmitigated disaster4, and the risk of that outcome should be our overriding concern.
Of course, we might also include parents and children.
If you’re interested in this topic, I recommend reading WPATH’s guidance on issues of transgenderism, available here: https://www.wpath.org/publications/soc
Some of the effects are reversable, while some are not. For example, a biological male who takes estrogen may grow breasts, and these will not go away, even if the patient stops taking estrogen: https://www.mayoclinic.org/tests-procedures/feminizing-hormone-therapy/about/pac-20385096
Read more about the effects of hormone therapy, and note that we haven’t even yet considered the (presumably more invasive) effects of surgical intervention: https://www.mayoclinic.org/tests-procedures/feminizing-hormone-therapy/about/pac-20385096